
Nova Scotia law protecting elderly ‘too weak’ and ineffective, advocacy group says - Halifax Examiner https://share.google/BlE2LnncBf8mAxAcI
Susan Charlton, MN, and I are members of ACE (Advocates for the Care of the Elderly). We wrote an open letter to Premier Houston which was sent to the media, MLA's and party leaders today from ACE. Both Susan and I had much loved parents who were badly abused in Nova Scotia nursing homes. We wrote the letter from the perspective of abused residents because they are invisible - unseen and unheard. Here is the letter:

Open Letter to: Premier Tim Houston, CC Minister Barbara
Adams
From: Abused Nursing Home Residents*
Dear Premier Houston,
Did you know that reports of abuse to the provincial
government’s Protection for Persons In Care have tripled in the last ten years,
now reaching over 600 per year? That the percentage of abuse reports
investigated has been cut in half? That confirmed abuses noted in the Act have
been denied an investigation?
It breaks our hearts to let you know that this is just the
tip of the iceberg. Our abuses are horrific. We’ve been left screaming in pain
and begging for help for days. We’ve been pushed to the floor by staff and
died, without police involvement. We’ve experienced the agony of bone deep
pressure sores, almost always preventable, and told there was no neglect. Tragically
there are many more incidents.
We have tried looking for help in the conventional places,
Police and Protection for Persons In Care, but it isn’t working. There are
virtually no consequences for abusing us, even for facilities with yearly and
even more frequent confirmed abuses. The Protection for Persons In Care Act,
passed in 2004, enables fines of up to $30,000 for corporate abusers. Can you
guess how many fines have been levied? None. Protection for Persons In Care (PPC)
has claimed in the media that abusing us doesn’t contravene the Act. PPC’s
director, Robert Lafferty, wrongly claims that NS’s legislation is the
strongest in Canada. Do you understand how painful this is to us? Abusing us
doesn’t contravene the Act and the director of the division responsible to
protect us proudly touts it as the strongest in Canada.
Our children, no longer young themselves, have researched
all of the Canadian provincial and territorial protective legislation related
to nursing home residents. They’ve also acquired a legal brief challenging
PPC’s interpretation of the Act and outlining it’s problems. Our legislation is
weak. There are holes in it you can drive a truck through. Sadly, even this
weak legislation is further watered down by failure to use the tools that are provided.
Dieticians are investigating physical abuse and writing reports with irrelevant
information about what victims did or didn’t eat, while screening cuts,
preventable falls and medical negligence out of the investigations. Our
children who witnessed our abuse and suffering were denied their right,
established in policy, to be included in investigation interviews. There’s
more, much more and we beg you to give us the legislation that will protect us.
Adding to the problem, one police department told us that
Protection for Persons In Care lets them know if potential criminal activity
has occurred. Protection for Persons In Care tells us that Police decide
whether criminal activity has occurred. The result? We can’t find any records
of criminal charges related to the hundreds of confirmed abuses that are on the
record. We suffer in silence, invisible, no justice or closure. We desperately
pray that you will see the need for better legislation to protect us.
Legislation equal to Nova Scotia’s Animal Protection Act would be a huge
improvement for us.
Please consider, “The quality of society is judged by how it
treats its elderly”. Pope Francis
Our children are advocating and researching for us. They’ll
present their full report in the fall of 2025. Please direct that staff
prepares stronger protective legislation and correctly implements the
legislation we have. Here are some of the research findings comparing Nova
Scotia’s legislation to other provinces and territories:
|
Legislation |
Some Canadian
Provinces and Territories |
Nova Scotia
PPC Act |
|
Clear
definitions - what abuse is and isn’t, included in the ACT. Clearly
defined Offenses. |
Yes |
No |
|
Description of
when and how police are involved in cases at the Inquiry Stage |
Yes |
No |
|
Appeal process |
Yes |
No |
|
Mandatory
fines for repeat offenders |
Yes |
No |
|
Minimum
qualifications for investigators required |
Yes |
No |
|
Transparency,
a degree of independent oversight |
Yes |
No |
|
Licenses can
be revoked if noncompliance** |
Yes |
See note |
*Written for abused residents by
Susan Charlton, MN and Carol Macomber, BDes
** Nova Scotia currently has
the ability to revoke licenses, but won’t, saying they can’t close nursing
homes. Other jurisdictions do this by naming a temporary administrator until
the issues are resolved.

Comparison, Nova Scotia’s Protection of Persons in Care
Act, 2007 and Animal Protection Act, 2018
January, 2025, prepared by Carol Macomber
|
|
NS Protection
of Persons in Care
Act, 2007 |
NS Animal
Protection Act, 2018 |
|
1.
Is
it explicitly stated that subjects can’t be left in pain? |
No |
Yes |
|
2.
Is it explicitly stated that subjects must
have adequate ventilation and protection
from heat or cold? |
No (nursing
home residents may be without air conditioning, in small rooms, in heat
waves.) |
Yes |
|
3.
Are
minimum professional qualifications for investigators/inspectors addressed? |
No |
Yes |
|
4.
Does the Act address potential conflict of
interest? |
No |
Yes |
|
5.
Does
the Act require an annual, publicly available report? |
No |
Yes |
|
6.
Does the Act require that investigators /
inspectors are special constables? (Special constable status enables the
investigator / inspector to lay charges.) |
No |
Yes |
|
7.
Does
the Act address repeat offenders? |
No |
Yes |
|
8.
Does abuse contravene the Act? |
No, according
to Protection of Persons in Care staff only failing to report abuse
contravenes the Act. Our legal opinion states otherwise. |
Yes |
|
9.
What
penalties are enabled? |
·
Up
to $2,000 fine, individual ·
Up
to $30,000 fine, corporation |
·
1st
offence, up to $25,000 fine and /or up to 6 months imprisonment ·
2nd
offence, up to $50,000 fine and / or up to 6 months imprisonment ·
3rd
or subsequent offence, $75,000 and / or up to 2 years imprisonment |
|
10.
Are the penalties re #9 above ever employed? |
No |
Yes |

Mom and I
This is my mother Margaret Macomber's final investigation report regarding her abuse at Shannex's Cedarstone Enhanced Care in Truro, Nova Scotia. It was prepared by Protection of Persons in Care, a division of the provincial Seniors and Long Term Care department. Some points are misleading, i.e. despite my clarification it states that I was indecisive about my mother going to hospital when in fact the Cedarstone staff told me they would get help more quickly and the hospital would be many hours, so I followed their advice still believing they wanted to help. (I've since learned in reading reports of abuse in Shannex facilities that other families have been discouraged from taking their loved one to hospital in cases of abuse. Perhaps it's related to the fact that the hospital reported the abuse in mom's case to Protection of Persons In Care.)
While my opinion / percepton is that the investigation and report were somewhat biased in Shannex's favour, it does shed light on the incident and confirm that abuse occurred. If there are other people who are willing to share their experience with Protectionn of Persons in Care I would love to hear your stories, good or bad. Did you make a complaint that wasn't investigated? It was investigated but abuse was determined unfounded despite evidence to the contrary? It was investigated and you're satisfied with the outcome regarding the findings and consequences? Please contact me at carol@fivefires.ca, subject line Abuse, if you have knowledge to share confidentially or publicly.
The thing about this incident that haunts me is that many of the same facilities, for profit corporate chain facilities, are repeatedly documented as abusing helpless seniors while facing no consequences. You read that right. They are profiting but are not required to pay the fines provided in law or criminally prosecuted. Ever. Some individual nursing homes belonging to the corporate chains have as many as twelve confirmed abuses from March 2017 to March 2024.
Please forgive the formatting. It's converted from a pdf so difficult to manage.
THE REPORT:
May 7, 2024 carol@fivefires.ca
Carol Macomber
SDM for Margaret Macomber
Dear C Macomber:
Re: Final Investigation Report - File #: CEDA-2023-10
On September 21, 2024, a report was made under the Protection for Persons in Care Act (PPCA) as outlined in the Final Investigation Report.
After a full investigation, the PPCA Office has concluded that the reported allegation is founded.
A copy of the final report is enclosed for your review.
If directives have been issued to the administrator of the health facility, the administrator is required to submit an action plan to address the directives If no directives were issued to the administrator, this file will be closed.
Staci Corbett, RD
Investigation and Compliance Officer
Department of Seniors and Long Term Care
OVERVIEW:
• On September 21, 2023, a report was received under the Protection for Persons in Care Act alleging failure to provide adequate nutrition, care, medical attention or necessities of life without valid consent as defined in section 3(1) (g) of the Regulations.
• It was alleged that the affected resident did not receive adequate medical attention during a period of severe pain and discomfort.
• It was determined that there were reasonable grounds to conduct an investigation pursuant to section 8 (2) of the Protection for Persons in Care Act.
• The investigation included interviews with relevant parties. The resident’s chart, care plan, Medication Administration Records (MARs), and other related documents were reviewed as part of the investigation.
SUMMARY OF INFORMATION COLLECTED:
1. It was reported that on September 16, 2023, the affected resident began showing signs of discomfort, displayed by shouting for help, moaning and rubbing their chest.
2. A progress note dated September 16, 2023 at 22:21h states:
“Resident was unsettled the whole night, keeps on shouting for help but relieves for a while when sipping water. Cannot stay still on bed (keeps on moving- risk for fall) and rubs their chest when shouting for help. Ensured safety, endorsed.”
3. Upon review of the affected residents Medication Administration Record (MAR) for September 16, 2023, the affected resident was given regularly scheduled acetaminophen at 1635h and 1942h.
4. Staff # 1 reported that they had come onto the unit for the first time on September 16, 2023, and were not familiar with the affected resident. Staff # 1 reported that care staff reported the affected resident’s behaviour as abnormal but as the affected resident would settle with sips of water, they continued with comfort care.
5. Staff # 1 reported that they did obtain a set of vitals for the affected resident and informed a responsibility nurse of the affected resident’s behaviour on the evening of September 16, 2023; however, there is no documentation to support this.
6. Staff # 2 reported that when they came on day shift on September 17, 2023, it was their first day shift since the affected resident was admitted to the facility on September 1, 2023. Staff # 2 reported that the affected resident was not eating well that day, which was reportedly not abnormal. Staff # 2 reported they informed a supervisor that the affected resident just wanted to stay in bed and was not wanting to consume food or supplements.
7. Staff # 2 reported that they asked the affected resident if they were in pain, to which the affected resident replied “no”, and that they just wanted to stay in bed.
8. A progress note in the affected resident’s chart on September 17, 2023 at 1733h states:
“Throughout the weekend resident has not been eating well- maybe 25% of meal consumed, refused to eat and would holler if was brought to the dining room for mealtime and request to be taken back to their room... Meal tray was provided in the room but with the same outcome only consuming 10% of resource ordered and not finishing. Talked to (staff) and was decided to send urine sample for assessment to the laboratory Monday (tomorrow), will endorse.”
9. Staff # 2 reported that they took the affected resident’s temperature and recalled it being in the normal range; however, there is no documentation to support this.
10. Staff # 3 reported coming onto day shift on September 18, 2023, and being told in report that the affected resident was in pain from the night before. Staff # 3 reported that the affected resident was moaning in pain but was not able to pinpoint where the pain was located.
11. It was reported that when the affected resident’s Substitute Decision Maker (SDM) came in to visit on September 18, 2023, at approximately 1030h that the affected resident was “screaming in pain, guttural screams”, and that they pressed the call bell to alert staff. It was reported that when staff came to the affected resident’s room, the SDM asked them to help the affected resident and was told that the pain started last night and that they would have to call the doctor to get an order for additional pain medication. The SDM reported that they were not contacted by the facility to be alerted of the affected residents change in health status, from the night before.
12. A progress note in the affected residents chart from September 18, 2023 at 0800h states
“Around 8 in the morning, resident was out in the dining room for breakfast. Writer noted resident was restless and agitated while on (their) chair and was shouting. Writer tried to offer porridge but resident refused. Resident was asked if they has any pain but doesn’t respond. V/S taken of 166/91, P: 86, R:26, T:36, O2 sat 97%. Writer tried to give their morning pills but resident refuse. Resident was assisted back to their room and was put to bed and did rested well. Around 1030, SDM came in and resident was starting to get restless again telling (their) SDM (they are) in pain. PRN Tylenol was given with a brief relief. Writer asked the SDM if she wanted to transfer to hospital and said yes but then took it back and just wants to give comfort measures and requested injectable medications for pain. Writer and RN (initials) tried to call (doctor) multiple times to get an order for morphine but couldn’t get a hold of (doctor). Writer and RN (initials) faxed Dr. regarding residents condition. SDM was frustrated on why we couldn’t get the doctor right away and verbalized “ this is inhumane” and “ I won’t think twice of publicizing this situation”. A dark colored blood was seen after Tylenol suppository was given. Resident did settle afterwards. Writer called 911 and asked if they can give emergency morphine as we couldn’t get an order for it. EMS came in around 1500H and assessed resident. Vital signs are within normal limit, ECG was taken, morphine SQ was given. SDM then decided to bring resident to the hospital. At 1530h, resident left facility for the hospital.
13. The affected resident was transferred to hospital at approximately 1530h on September 18, 2023.
14. A triage assessment from September 18, 2023, was observed from the emergency department as part of the investigation and stated the following:
“1630h- 99f w/ abdominal/chest pain since yesterday. Was yelling and moaning in pain on arrival but has received 5mg morphine sq and quite comfortable now.”
15. A history and physical document, from the receiving hospital, was reviewed as part of the investigation and stated the following:
“Reason for Admission- probable acute MI
General- Affected resident was distressed with pain on presentation. The morning after admission, they are sleeping deeply with pain medications having been given.
Plan- this 99 year old (pronoun) seems to have had some significant event, likely cardiovascular event with their elevated troponin. Their lactate was also elevated…”
ADDITIONAL INFORMATION COLLECTED:
16. Upon review of the affected resident’s Medication Administration Record (MAR) from the facility, it was observed that Tylenol (acetaminophen) was a regularly scheduled medication and there were no other medications ordered for pain.
PRN (as needed) Medication Administration Records (MARs) were requested as part of the investigation; however, the investigator was informed that the affected resident did not have any PRN medications prescribed.
17. Staff # 3 reported that the affected resident’s Pathway of Care was limited interventions / No CPR. Staff # 3 also reported that the SDM for the affected resident was indecisive on whether or not they wanted the affected resident transferred to hospital, or to stay at the facility and kept comfortable.
18. A three-day admission assessment was observed as part of the investigation and included a section to assess pain. It was completed for September 2, 3, 4, 2023 and indicated that the affected resident did not complain or show evidence of pain nor had sudden, acute flare ups of pain.
19. Staff # 4 reported that there was a delay in contacting the facility physician as staff working were calling and faxing the physician’s office number and not their cell phone. It was reported by staff interviewed that they did not have any additional phone numbers or way to contact the physician aside from the phone number to the physician’s office.
20. It was reported that as part of the internal investigation conducted by the facility, it was determined that the process for contacting the facility physician was updated with direction for staff to request a transfer to the facility physician’s cell phone in the case of an emergency when calling the physician’s office number.
21. It was reported by all staff interviewed that the affected resident’s substitute decision maker (SDM) was not made aware of the affected resident’s health status from September 16-18th, 2023, until they arrived at 1030h on September 18, 2023.
22. The affected resident was unable to participate in the investigation.
ADDITIONAL INFORMATION:
• The Medication Administration Record (MAR) for the affected resident was reviewed as part of the investigation. It was noted that their regularly scheduled Tylenol was documented on the MAR as being refused by the affected resident on September 17, 2023, at 0800h, 1200h, 1600h and 50% taken at 2000h. Additionally, the 0800h dose of Tylenol was documented as being refused on September 18th, 2023, as well.
• According to the facility’s Medication Management Policy, if the resident refuses a medication or treatment, continue to make attempts to assist with the medication or treatment. However, if you run out of the window of time for taking the medication or treatment (refer to medication administration SOP) and the resident still declines, place a circle in the box, write your initials inside this circle, and chart the reason for the refusal in the notes on the back of the MAR or TAR.
Notify the appropriate person of this refusal.”
• According to the facility’s Pain Management Policy, any change in resident condition that may be contributed by pain, must trigger a pain assessment to be completed along with care planning for pain in collaboration with the interdisciplinary team and the Substitute Decision Maker (SDM). A pain assessment for the affected resident was completed on admission, however, subsequent pain assessments were not observed as part of the investigation.
• It was documented in the affected resident’s progress notes that a skin tear occurred on their left shin on September 7th, 2023. This was documented and treated and SDM notified. Additionally, on September 10, 2023, a progress note indicated a skin laceration was observed on the affected resident’s lower left leg and was treated according to the wound care policy. On September 16, 2023, a progress note indicated the affected resident had a scratch on their left backside, (2.3 inches) and purplish bruises to both arms and legs.
• A progress note from the affected resident’s file on September 18, 2023 at 0455h states:
“At around 0340h CCA on duty (initials) informed writer that resident has wound on (their) leg and it is bleeding. Upon assessment writer noted blood on the bedsheet and on the left side rail. Multiple skin tear was noted on the left lower limb and with light bleeding, no swelling noted. Writer cleansed wound with NSS, painted with betadine, Covered with non-adherent dressing and wrapped with a kling…”
RESPONSES TO PRELIMINARY INVESTIGATION REPORT:
A response to the Preliminary Investigation Report was not received from the facility.
A 23 page response to the Preliminary Investigation Report submitted by the Substitute Decision Maker for the affected resident has been reviewed and considered in the investigation. The response included questions, comments, and points of clarification, some of which have been added above in “Additional Information”. While not an exhaustive list, some of the relevant responses are summarized below:
The SDM reported that on September 18, 2023:
“I arrived at Cedar Stone at 10:30 am and heard (affected resident) screaming as I came through the doors to (their) wing. I got to (their) room and (their) door was closed. Rushing to (their) bedside I grabbed the call button and rang for help, assuming that staff didn’t know that (affected resident) was in severe distress. When I asked staff to help (affected resident) they said that (they) refused to take (their) acetaminophen that morning. Nothing else was offered. (Their) ‘refusal’ to take (their) medication was the only explanation provided for (their) condition. I, completely untrained in medicine, could see (affected resident) wasn’t capable of taking (their) medication (they later vomited). I asked that staff get injectable pain medication and medical attention immediately. (Affected resident’s) legs were badly cut when I arrived, adding to (their) pain. Staff told me (affected resident) had cut them on the bed rails when thrashing in pain. The bed rails were down when I arrived and (affected resident) was still thrashing.
(Affected resident’s) pain continued with the exception of two brief respites until approximately 3:00 pm.
Although (they) couldn’t swallow medication, acetaminophen suppositories weren’t offered until hours after I started begging for help. When the suppository was provided staff noted that (affected resident) had blood in (their) rectum. Injectable pain medication wasn’t provided until I threated to post video of (affected resident) screaming and writhing in pain to social media. EMT’s were there within minutes and immediately recognized that it was an emergency.”
FINDINGS:
On September 16th, 2023, it was documented that the affected resident was shouting for help and rubbing their chest, which was reported as abnormal behaviour by care staff. The following day, a staff member reported to their supervisor that the affected resident was not eating well and hollering when brought out to the dining room. It was reported that the affected resident was asked if they were in any pain and reportedly stated “no”. It was reported that staff obtained vitals on multiple occasions as part of their assessment of the affected resident, however, there is no evidence to support this nor evidence to support that the affected resident was asked if they were in pain and replied “no”.
On review of the Medication Administration Record (MAR) it appears as though the affected resident refused their regularly scheduled Tylenol during three medication passes on September 17, 2023, and only took 50% of the dose at 2000h. On September 18, 2023, it was reported that the affected resident was in pain from the night before, moaning in pain, however, there is no documentation to support that the affected resident was experiencing pain or any evidence of investigation into this pain.
On September 18, 2023, the Substitute Decision Maker (SDM) reported that when they arrived at the facility, the affected resident could be heard screaming from down the hall and was in obvious pain in their room. The SDM reported that they were told the pain began the night before, September 17, 2023. The SDM was not made aware of any change in condition beginning on September 16, 2023, until they arrived at the facility on September 18, 2023, at approximately 1030h. The facility physician was unable to be reached via phone and fax after several attempts, and EHS was called, at the insistence of the SDM, to administer injectable pain medication. The admitting hospital noted that the affected resident was yelling and moaning in pain on arrival, which is supported by the SDM’s account of the events, however, there appears to be a discrepancy between documentation of the affected resident’s pain from the facility and the accounts from the SDM and admitting hospital. It was noted that the affected resident experienced a probable acute MI after the admitting hospital’s investigation.
Although there is a discrepancy between what was reported and documented by the SDM, admitting hospital and the facility, it can be concluded that the affected resident began experiencing some level of discomfort on September 16th, 2023, as evidenced by rubbing their chest and shouting out for help, until being transferred to hospital on September 18, 2023 at 1530h. Documentation detailing the affected resident’s pain and discomfort was limited, pain medication refusals were not reported to a charge staff or documented in the chart, the affected resident’s SDM was not notified of a change in condition, or medication refusals, until they arrived and witnessed the affected resident in pain and discomfort. Vitals were reportedly obtained on multiple occasions, however, there is no documentation to support this. Additionally, according to the facility’s pain management policy, a change in condition that may be contributed to pain, must trigger a pain assessment. A pain assessment was completed on admission for the affected resident on September 2,3, and 4, 2023 which indicated that the affected resident did not complain or show evidence of pain nor had sudden, acute flare ups of pain, therefore the change in behaviour noted on September 16, 2023, should have triggered a pain assessment to be completed. There was no evidence of a completed pain assessment after September 4, 2023.
Although there is evidence that care staff were completing tasks related to care for the affected resident, several staff reported that they were unfamiliar with the affected resident, their baseline, or usual behaviours, which contributed to a failure to recognize and act upon a change in condition and behaviour of the affected resident beginning on September 16, 2023. There is a lack of documentation and follow-up related to vitals, pain assessments, medication refusals and reports to supervisors. Additionally, there was a failure to provide timely communication to the SDM and facility physician contributing to the affected resident experiencing pain and discomfort for several hours.
As a result of the lack of overall coordination and oversight of care, the allegation of failure to provide adequate nutrition, care, medical attention or necessities of life without valid consent as defined in section 3(1) (g) of the Regulations is founded.
DIRECTIVES:
1. During the investigation, it was reported that staff obtained vitals on multiple occasions, however, they were not documented in the affected resident’s chart. Additionally, descriptions of pain and health status changes, interventions related to mitigating pain and medication refusals were not documented and/or did not follow facility policy for documentation standards. As such, it is required that the Administrator ensures all staff involved in the allegation are provided with education related to the Medication Management Policy and documentation standards for clear, timely and accurate documentation.
2. During the investigation interviews, it was reported that staff relayed pertinent information to other staff members and/or supervisors about the affected resident’s condition, however, progress notes only indicated that information was “endorsed” with no further detail. The Administrator shall ensure that the process for sharing report and information with oncoming shifts and/or supervisors is reviewed, and documentation shall reflect who the information is reported to.
3. During the investigation, there is evidence that the affected resident experienced a change in health status ie: pain. There was no evidence that the Substitute Decision Maker (SDM) was notified of the change in health status. As such, the Administrator shall ensure that relevant staff, including facility management, review the facility’s SDM informing process, to ensure SDMs are appropriately, and accurately, informed of all concerning information involving residents in a timely manner, and that such communication is documented on resident charts.
4. According to the facility’s Pain Management Policy any change in resident condition that may be contributed by pain, must trigger a pain assessment to be completed along with care planning for pain in collaboration with the interdisciplinary team and the Substitute Decision Maker (SDM). Staff failed to recognize or act on the change in condition of the affected resident and therefore did not complete a pain assessment. The Administrator shall ensure that all staff involved are provided with education on the Pain Management Policy, conducting pain assessments and recognizing changes in resident condition.
5. Despite individual staff documenting concerns identified with the affected resident, there was a lack of overall coordination of care and accountability. Staff reported being unfamiliar with the affected resident. The Administrator shall ensure that the process for coordination of care, including reporting, oversight and decision making is reviewed to ensure all staff are familiar with their role in continuity of care for residents.



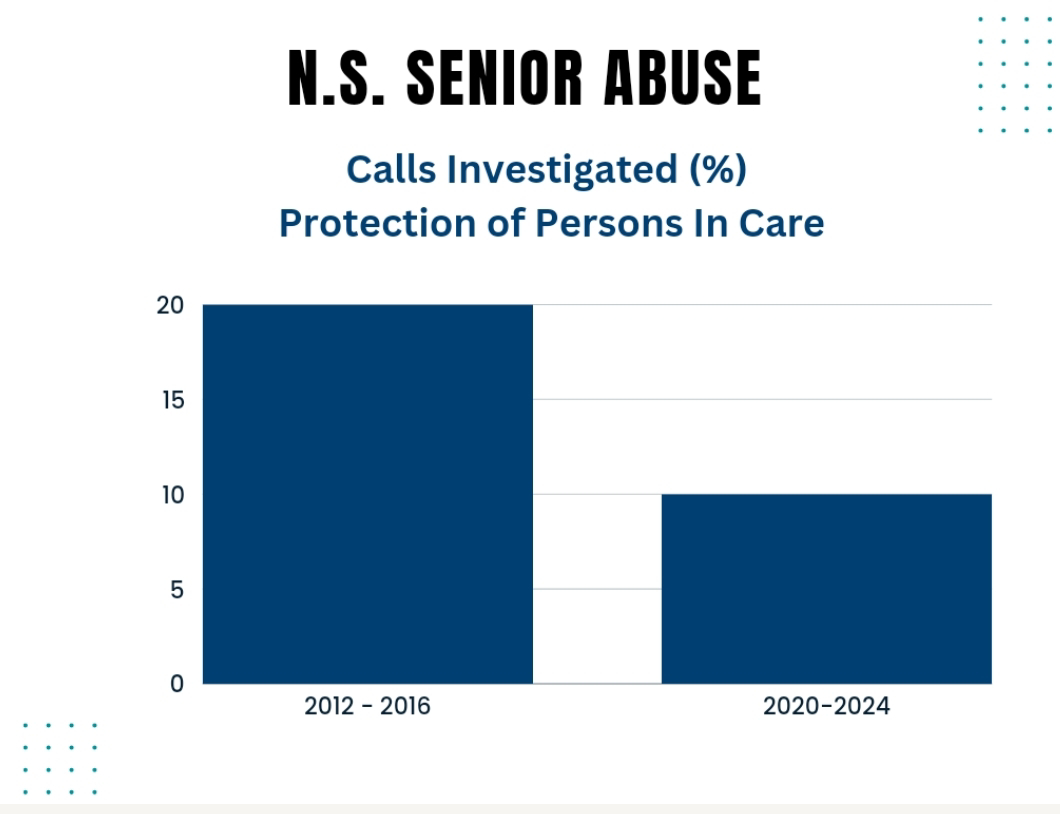
HOW MUCH ABUSE IS OCCURRING?
1. Reviewing senior abuse media coverage from 2017 it becomes apparent that reports of abuse have more than doubled in the last ten years (approximate numbers in graph 1 above). The percent of reports investigated has almost been cut in half (graph 2 above).
2. There have been approximately 245 confirmed cases of senior abuse in Nova Scotia in the last seven years. These include physical and sexual assaults, extreme unmanaged pain, deaths from untreated injuries and more.
WHO ARE THE WORST OFFENDERS?
1. Comparing all nursing homes in Nova Scotia with more than 100 beds, residents are approximately 65% more likely to be abused in a for profit nursing home than a not for profit or public nursing home. All of these for profit facilities with more than 100 beds belong to either Shannex or GEM Health.
2. The top five facilities with the most confirmed abuses over the last seven years are all for profit facilities belong to Shannex or GEM Health:
3. Tim Houston's Conservative government, knowing this, gave Shannex a sole sourced contract for $120 million to provide more beds.
WHO PROTECTS? ARE THEY EFFECTIVE?
1. Seniors in long term care are entitled to the same protective services that all Canadian citizens have. They aren't receiving this essential human right.
2. The provincial government is responsible for protecting seniors in nursing homes via the Protection of Persons in Care Act. They provide an investigation service through the Protection of Persons in Care division of Seniors and Long Term Care. It would be impossible to convey how bizarre this 'service' is without experiencing it first hand. They investigate, conduct interviews, review documentation, photos and video. Months go by, preliminary reports are generated, more evidence is examined and then, regardless of a finding of abuse - nothing meaningful happens. There are no consequences to abusing our most vulnerable and loved family members. You read that right. I stand behind the statement 100%. It sounds unbelievable but it's true. I'll provide more detail in a future post.
In the meantime, as an example of the service's lack of accountability, here are some pages I reviewed from past freedom of information releases of investigation reports. The thirty five reports I reviewed consistently looked like this:



Here's a very thorough article about nursing home resident abuse in Nova Scotia. Thank you Jennifer Henderson and the Halifa...

